
Radial Club Hand
Radial Club Hand
रेडियल क्लब हैंड - पूरी जानकारी | हिंदी & English Guide
Complete Guide to Radial Club Hand | Hindi & English
Radial Club Hand क्या है?
What is Radial Club Hand?
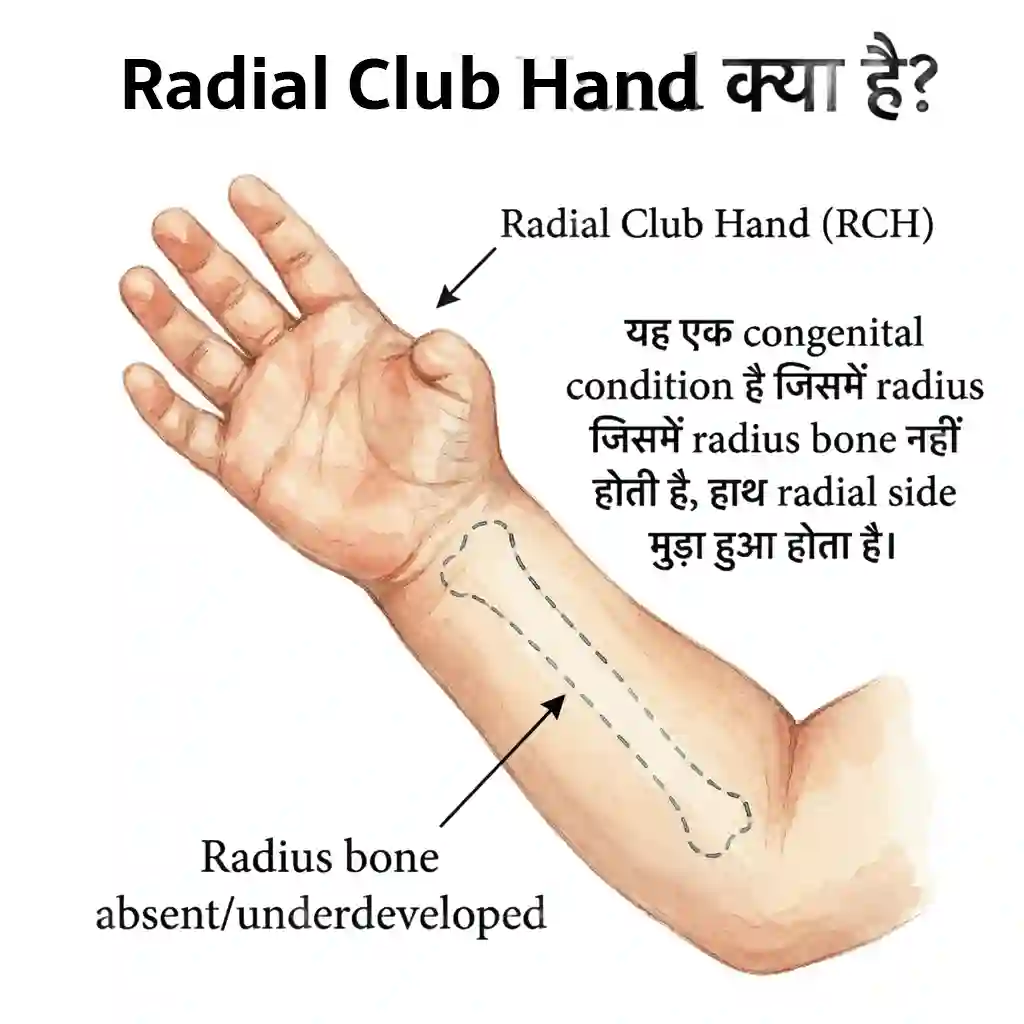
Radial Club Hand (RCH) एक congenital condition है जिसमें radius bone (अंगूठे वाली side की forearm bone) absent या underdeveloped होती है। इससे hand radial side की तरफ मुड़ा हुआ (deviated) होता है।
🎯 Key Facts!
Rare condition! 1 in 30,000 births। Also called Radial Ray Deficiency या Longitudinal Radial Deficiency। Spectrum condition - mild से severe। Often associated with thumb abnormalities। May be part of syndrome (VACTERL, TAR, Holt-Oram)। Early treatment crucial! Surgical correction possible!
📊 Key Statistics:
जन्मों में
दोनों हाथ
सर्जरी उम्र
सुधार
🧠 What Happens Anatomically?
Radius bone absent या partially developed।
Effects: Hand radially deviated (bent towards thumb)। Thumb absent या hypoplastic। Ulna bowed। Wrist unstable। Limited forearm rotation। Elbow stiffness।
Associated findings: Muscle deficiencies (radial side)। Blood vessel abnormalities। Nerve issues (radial nerve)।
🔑 Important: Early diagnosis essential! Better outcomes with early intervention। Surgical timing crucial!
⚠️ Common Misconceptions:
- Myth: केवल cosmetic problem। Fact: Functional impairment significant!
- Myth: Surgery cure करेगी। Fact: Improves but doesn't make hand "normal"!
- Myth: Self-correct होगा। Fact: Treatment needed - won't improve spontaneously!
- Myth: केवल hand problem। Fact: May be part of syndrome - need full evaluation!
Radial Club Hand (RCH) is congenital condition with radius bone absent or underdeveloped. Hand deviated radially towards thumb side.
🎯 Key Facts!
Rare condition! 1 in 30,000 births. Also called Radial Ray Deficiency. Spectrum from mild to severe. Early treatment crucial!
📊 Stats:
RCH के प्रकार (Types)
Types of Radial Club Hand
🎯 4 Types - Bayne Classification!
Type I (Mild) → Type IV (Severe) | Based on radius development
📋 RCH Types Detailed:
Type I - Distal Radial Deficiency
Mildest form! Distal radius shortened। Proximal radius normal। Minimal hand deviation। Growth plate (physis) affected। Often requires no surgery या minimal intervention। Best prognosis। May need only splinting।
Type II - Hypoplastic Radius
Radius present but small! Both ends of radius abnormal। Severely shortened। Moderate hand deviation। Thumb usually hypoplastic। Requires centralization surgery। Functional improvement possible।
Type III - Partial Absence
Only part of radius present! Usually distal portion absent। Significant deformity। Thumb often absent। Hand severely deviated। Requires complex surgery - centralization/radialization। Ulna bowed।
Type IV - Complete Absence
MOST SEVERE! Radius completely absent। Extreme radial deviation। Thumb absent। Severe muscle deficiencies। Maximum deformity। Requires multiple surgeries - staged approach। Challenging management।
✅ Associated Thumb Abnormalities (Common!):
- Thumb Hypoplasia: छोटा, underdeveloped thumb (common in Type II-IV)
- Thumb Absence: complete absence (Type III-IV)
- Triphalangeal Thumb: तीन phalanges instead of two
- Floating Thumb: thumb केवल skin से जुड़ा
- Classification: Blauth classification (Grade 1-5) for thumb severity
🎯 4 Types - Bayne!
Type I (Mild) → IV (Severe)
Types:
Type I
Distal radius short. Minimal deviation. Often no surgery needed.
Type II
Hypoplastic radius. Moderate deviation. Surgery required.
Type III
Partial absence. Severe deformity. Complex surgery.
Type IV
Complete absence. Most severe. Multiple surgeries.
लक्षण और निदान
Symptoms & Diagnosis
Usually diagnosed at birth! Visible deformity। Range: mild deviation से severe malformation।
👀 Clinical Features:
Hand Position
Radially deviated! Hand bent towards thumb side। Severity varies by type। Unable to straighten। Wrist unstable। Forearm shortened। Limited supination/pronation।
Thumb Abnormality
Often absent या hypoplastic! Type II-IV: thumb severely affected। May be floating thumb। Triphalangeal thumb। Functional loss of pinch and grasp।
Muscle Deficiencies
Radial side muscles absent! Brachioradialis absent। Thenar muscles hypoplastic। Weakness in radial deviation। Limited wrist extension।
Bone Abnormalities
Radius absent/short! Ulna bowed (curved)। Shortened forearm। Growth discrepancy। Elbow stiffness। Carpal abnormalities।
🔍 Diagnosis Process:
Medical Assessment:
1. Clinical Exam: Inspection - hand position, thumb status। Palpation - feel radius। ROM assessment। Neurovascular exam।
2. Imaging: X-rays (confirm type, ulna bow)। Ultrasound (infants - cartilaginous structures)।
3. Classification: Bayne classification (Type I-IV)। Thumb classification (Blauth Grade 1-5)।
4. Associated Evaluation: Full skeletal survey। Cardiac echo। Renal ultrasound। Blood counts (TAR syndrome)। Genetic testing if syndromic।
⏰ Diagnosis: Usually at birth! X-rays confirm। Full workup for syndromes!
⚠️ Associated Syndromes (Must Rule Out!):
- VACTERL Association: Vertebral, Anorectal, Cardiac, TE fistula, Renal, Limb abnormalities
- Holt-Oram Syndrome: Cardiac defects (ASD, VSD) + radial deficiency
- TAR Syndrome: Thrombocytopenia (low platelets) + absent radius
- Fanconi Anemia: Bone marrow failure + radial defects
- Nager Syndrome: Facial abnormalities + limb defects
- Other: Chromosomal abnormalities, CHARGE syndrome
IMPORTANT: 40-60% have associated anomalies! Full evaluation essential!
Diagnosed at birth! Visible deformity. Severity varies.
Clinical Features:
Hand Deviation
Radially bent. Severity varies. Unstable wrist.
Thumb Issues
Absent or hypoplastic. Functional loss. Limited grasp.
Muscle Loss
Radial muscles absent. Weakness. Limited function.
उपचार और प्रबंधन
Treatment & Management
🏥 Multidisciplinary Team Approach!
Pediatric Orthopedic Surgeon + Hand Surgeon + Therapist + More!
Treatment goals: Improve function, appearance, और wrist stability! Treatment individualized based on type and severity।
🎯 Main Treatment Approaches:
1. Non-Surgical (Initial)
Early splinting/stretching! Passive stretching exercises। Serial casting (pre-surgical)। Goal: Soften tissues। Improve hand position। Prepare for surgery। Started in first months। Occupational therapy। Parent education।
2. Centralization Surgery
GOLD STANDARD for Type II-IV! Age: 6-12 months ideal। Procedure: Hand "centralized" over ulna। Soft tissue releases। Carpal alignment। Maintains wrist stability। Ulna osteotomy if severely bowed। Long-term splinting post-op।
3. Radialization Surgery
Alternative technique! Hand positioned over radial side of ulna। May preserve wrist motion better। Less recurrence। Newer approach। Requires expertise। Similar age timing। Post-op therapy essential।
4. Pollicization (Thumb)
If thumb absent! Index finger converted to thumb। Restores pinch and grasp! Done after wrist surgery। Age: 1-2 years। Complex procedure। Functional improvement significant। Dr. Gaurav Jain expert!
🔬 Advanced Technique: Paley's Ulnarization
🎯 Revolutionary Approach by Dr. Dror Paley!
Ulnarization एक modern technique है जो traditional centralization/radialization से different है। Advantage: Better motion preservation और less recurrence!
📋 What is Ulnarization?
Concept: Instead of centralizing hand over ulna, procedure creates a stable wrist by positioning carpus on the ulnar shaft while maintaining soft tissue balance। Different from centralization - focuses on functional wrist joint creation।
🔧 Surgical Technique:
- Soft Tissue Release: Radial-sided tight structures released
- Ulnar Alignment: Hand positioned on distal ulna - NOT shortening ulna!
- Wrist Stabilization: Carpal bones aligned with ulnar articular surface
- Muscle Rebalancing: Preserve all possible muscles - no ablation
- K-wire Fixation: Temporary pins maintain position during healing
- Age: Typically 6-12 months (same as centralization)
✅ Advantages of Ulnarization:
- Better Wrist Motion: Preserves more range of motion than centralization
- Less Recurrence: Lower rate of re-deviation (compared to centralization)
- Growth Preservation: Maintains distal ulnar physis (growth plate)
- Functional Joint: Creates more anatomic wrist joint
- No Ulnar Shortening: Unlike centralization - length preserved
- Better Grip Strength: Improved power grip capability
⚖️ Ulnarization vs Traditional Methods:
Centralization: Hand centered on ulna - often requires ulnar shortening। Higher recurrence। More wrist stiffness।
Radialization: Hand positioned on radial side of ulna। Better than centralization but still has limitations।
Ulnarization: Creates functional wrist joint without shortening। Best motion preservation। Lowest recurrence। Most anatomic reconstruction।
📊 Evidence & Outcomes:
Studies show: Ulnarization has superior wrist motion (40-60° vs 20-30° with centralization)। Recurrence rates: 10-15% (vs 30-40% centralization)। Patient satisfaction higher। Functional scores better। Long-term results promising।
⚠️ Considerations:
- Surgeon Expertise: Requires specialized training - not all surgeons perform
- Type Suitability: Best for Type II-IV radial club hand
- Post-op Protocol: Still requires splinting (but potentially shorter duration)
- Newer Technique: Less long-term data than centralization (but growing evidence)
🏥 Dr. Gaurav Jain evaluates each child individually और determines best surgical approach - centralization, radialization, या ulnarization - based on severity, anatomy, और individual factors। Modern techniques like ulnarization offer promising results!
✅ Surgical Stages (Typical Timeline):
- Birth - 6 months: Serial casting, stretching, soft tissue preparation
- 6-12 months: Centralization/Radialization surgery (optimal timing!)
- 1-2 years: Pollicization (if thumb absent)
- Later childhood: Tendon transfers (if needed), correction of recurrence
- Adolescence: Ulnar lengthening procedures (if significant shortening)
🔧 Post-Operative Care:
Splinting: Long-term (often years) - maintain correction।
Therapy: Occupational therapy - ROM, strengthening। Functional activities।
Monitoring: Regular follow-up। Watch for recurrence। Growth monitoring।
Recurrence: Common (up to 30%) - may need revision। Splint compliance crucial!
⚠️ Possible Complications:
- Recurrence: hand deviation returns (most common complication!)
- Wrist stiffness: limited ROM despite surgery
- Growth disturbance: ulnar bow may worsen
- Neurovascular injury: rare but possible
- Infection: surgical site infection
🏥 Team Approach!
Orthopedic Surgeon + Hand Surgeon + Therapist
Goals: Function + Appearance + Stability! Individualized treatment.
Treatments:
Splinting
Early stretching. Serial casting. Pre-surgical preparation.
Centralization
Gold standard. Age 6-12 months. Long-term splinting.
Radialization
Alternative technique. Better motion. Newer approach.
Pollicization
Thumb reconstruction. Age 1-2 years. Restores pinch.
🔬 Advanced: Paley's Ulnarization
🎯 Revolutionary Technique by Dr. Dror Paley!
Ulnarization is modern approach different from traditional centralization/radialization. Better motion + Less recurrence!
What is Ulnarization?
Concept: Creates stable wrist by positioning carpus on ulnar shaft while maintaining soft tissue balance. Focuses on functional wrist joint creation.
🔧 Technique:
- Soft tissue release - radial side
- Hand positioned on distal ulna - NO ulnar shortening
- Wrist stabilization - carpal alignment
- Muscle rebalancing - preserve all muscles
- K-wire fixation temporary
- Age: 6-12 months typically
✅ Advantages:
- Better wrist motion - preserves ROM
- Less recurrence - 10-15% vs 30-40%
- Growth preservation - maintains distal ulnar physis
- Functional joint - more anatomic
- No ulnar shortening - length preserved
- Better grip strength
⚖️ Comparison:
Centralization: Higher recurrence. More stiffness. Requires ulnar shortening.
Radialization: Better than centralization but limitations remain.
Ulnarization: Best motion preservation. Lowest recurrence. Most anatomic.
📊 Outcomes:
Studies: Superior wrist motion (40-60° vs 20-30°). Recurrence 10-15%. Higher satisfaction. Better function.
🏥 Dr. Gaurav Jain evaluates each child individually and determines best approach - centralization, radialization, or ulnarization - based on severity and anatomy!
विशेषज्ञ वीडियो
Expert Videos
डॉ. गौरव जैन द्वारा रेडियल क्लब हैंड के उपचार और प्रबंधन पर विशेषज्ञ जानकारी
Expert insights on Radial Club Hand treatment and management by Dr. Gaurav Jain
सामान्य प्रश्न (FAQs)
Frequently Asked Questions
Radial club hand क्या है? / What is radial club hand?
Radial club hand (RCH) एक congenital deformity है जिसमें radius bone (forearm की अंगूठे वाली side की bone) partially या completely absent होती है। Result: hand radially deviated (bent towards thumb side)। Also called Radial Ray Deficiency। Spectrum condition - mild से severe। 1 in 30,000 births। Often thumb भी affected। Early treatment essential!
Surgery कब? / When is surgery needed?
Type II-IV के लिए surgery usually needed! Optimal age: 6-12 months for centralization/radialization। Type I may need NO surgery। Pre-surgical stretching and casting first। Early surgery = better outcomes। Goals: correct deformity, improve function, stabilize wrist। Multiple stages often needed। Dr. Gaurav Jain expert in RCH surgery!
Centralization क्या है? / What is centralization?
Gold standard surgery for RCH! Procedure: hand को ulna के center में align करना। Soft tissue releases। Carpal bones repositioned। Wrist stabilized। Done at 6-12 months। Long-term splinting after। Recurrence possible। Improves function significantly। Alternative: Radialization (hand over radial side of ulna)।
Thumb का क्या होगा? / What about the thumb?
Thumb often absent या severely hypoplastic in Type II-IV! Treatment options: (1) Pollicization - index finger को thumb बनाना (if thumb absent) (2) Thumb reconstruction (if thumb present but hypoplastic) (3) No treatment (if thumb mildly affected)। Pollicization age: 1-2 years। Restores pinch and grasp। Functional results good!
Causes? / कारण क्या?
Usually unknown! Developmental abnormality during fetal development (4-8 weeks gestation)। Possible causes: (1) Genetic mutations (2) Chromosomal abnormalities (3) Vascular disruption (4) Teratogens (medications, environmental)। Often sporadic। 40-60% associated with syndromes (VACTERL, Holt-Oram, TAR, Fanconi)। Rarely familial। Not preventable in most cases!
Types? / कितने प्रकार?
Bayne Classification - 4 types based on radius development: Type I - Distal radius short (mildest)। Type II - Radius hypoplastic but present। Type III - Partial radius absence। Type IV - Complete radius absence (most severe)। Severity increases I→IV। Thumb abnormalities more common in III-IV। Treatment complexity increases with type!
Pre-surgical care? / सर्जरी से पहले क्या?
Important preparation! (1) Passive stretching exercises (2) Serial casting - progressive correction (3) Splinting - maintain stretch (4) Occupational therapy (5) Soft tissue mobilization। Started in first weeks/months। Goal: soften tight radial structures। Improve hand position before surgery। Better surgical outcomes। Usually 2-6 months pre-op preparation!
Function कैसा होगा? / What about hand function?
Depends on severity and treatment! Type I: near-normal function। Type II-III: good function with surgery। Type IV: functional but limitations remain। Pollicization greatly improves grasp। Wrist motion usually limited। Grip strength reduced। BUT - most children adapt well। Can perform daily activities। School, writing, feeding possible। Occupational therapy helps। Early intervention = best outcomes!
Recurrence? / फिर से टेढ़ा होगा?
YES - common complication! Up to 30% recurrence। Hand deviation returns। Causes: growth, muscle imbalance, inadequate soft tissue release, poor splint compliance। Prevention: strict splinting (years!), regular therapy, monitoring। If recurs: may need revision surgery। Radialization may have less recurrence। Splint compliance CRUCIAL to prevent recurrence!
Associated syndromes? / अन्य problems?
40-60% have associated anomalies! Common syndromes: VACTERL (heart, kidney, spine, GI), Holt-Oram (heart defects), TAR (low platelets), Fanconi anemia (bone marrow), Nager (facial)। MUST evaluate: cardiac echo, renal ultrasound, skeletal survey, blood counts। Genetic testing if syndromic। Full workup essential। Treatment may need coordination with multiple specialists!
Limb shortening? / हाथ छोटा रहेगा?
YES - forearm usually shorter on affected side। Radius absent = no radial growth। Ulna may be short too। Discrepancy increases with age। Bilateral cases: both short (less noticeable)। Unilateral: visible difference। Lengthening procedures possible in adolescence (rare)। Most adapt well। Cosmetic issue more than functional। Focus on function not length!
Post-surgery care? / सर्जरी के बाद देखभाल?
CRITICAL for success! (1) Cast for 6-8 weeks (2) Then long-term splinting - often until skeletal maturity! (3) Occupational therapy - ROM, strengthening (4) Activity modification initially (5) Regular follow-up - watch recurrence (6) Splint compliance ESSENTIAL - wear schedule gradually reduced। No compliance = recurrence। Parents must commit long-term!
Ulnarization क्या है? / What is ulnarization?
Modern surgical technique by Dr. Dror Paley! Different from centralization। Ulnarization creates functional wrist joint by positioning carpus on ulnar shaft WITHOUT shortening ulna। Advantages: (1) Better wrist motion (40-60° vs 20-30°) (2) Lower recurrence (10-15% vs 30-40%) (3) Preserves growth plate (4) More anatomic reconstruction (5) Better grip strength। Requires specialized expertise। Growing evidence shows superior outcomes। Dr. Gaurav Jain evaluates if suitable for each child!
Centralization vs Radialization vs Ulnarization? / कौनसा बेहतर?
तीन main surgical options! CENTRALIZATION: Traditional (most experience), hand centered on ulna, requires ulnar shortening, higher recurrence (30-40%), more stiffness। RADIALIZATION: Hand over radial side, better than centralization, lower recurrence। ULNARIZATION: Newest/advanced, best motion preservation, lowest recurrence (10-15%), no ulnar shortening, most anatomic, requires expertise। Choice depends on: Type severity, surgeon experience, anatomy, family preference। All need long-term splinting। Dr. Gaurav Jain discusses options with families!
Centralization vs Radialization? / कौनसा बेहतर?
Both options! Centralization: traditional, hand over ulna center। Radialization: newer, hand over radial side of ulna। Radialization advantages: better wrist motion, less recurrence, preserves ulnar physis। Centralization: more experience, established results। Choice depends on severity, surgeon preference, anatomy। Both require long-term splinting। Results comparable। Dr. Gaurav Jain evaluates best option for each child!
School और activities? / पढ़ाई और खेल?
Most children attend regular school! Writing: may use adaptive devices। Sports: participation possible with modifications। Swimming: excellent activity। Activities needing two hands: may need adaptations। School support: occupational therapy, assistive technology। Intelligence: NORMAL unless syndromic। With proper management: education, employment, independence all possible। Many lead full, productive lives!
Long-term outcome? / भविष्य कैसा?
Generally GOOD with early treatment! Type I: excellent। Type II-III: good functional outcomes। Type IV: functional but limitations। Most achieve independence। Can perform ADLs (activities of daily living)। Employment possible। Cosmetic concerns may persist। Psychological support important। Bilateral cases adapt well (use both hands together)। Early surgery + compliance + therapy = best results। Life expectancy normal (unless syndromic)!
Which specialists needed? / कौन से doctors?
Multidisciplinary team! (1) Pediatric Orthopedic Surgeon (Dr. Gaurav Jain!) - primary surgeon (2) Hand Surgeon - specialized care (3) Occupational Therapist - function, ADLs (4) Geneticist - syndrome evaluation (5) Cardiologist - if cardiac defects (6) Other specialists - based on associated problems। Regular coordination essential। Team approach = best outcomes!
Treatment cost? / खर्चा कितना?
Varies by type and procedures! Centralization/Radialization/Ulnarization: ₹1,50,000-3,50,000। Pollicization: ₹1,00,000-2,50,000। Therapy sessions: ongoing cost। Splints/casts: additional। Multiple surgeries may be needed। Government schemes available। NGO support। Insurance coverage। Prioritize early intervention। Long-term investment but worth it। Discuss with Dr. Gaurav Jain - customized plan!
Bilateral होने पर? / If both hands affected?
60% bilateral (both hands)! Challenges: no "normal" hand to compare। Functional demands higher। Staged surgery - one hand first, then other। Timing: allow recovery between surgeries। Advantages: adapt to use both hands together। Symmetrical। Disadvantages: both hands limited। BUT - with therapy: most achieve independence। Bilateral actually adapt better than unilateral in some ways!
Prevention possible? / रोकथाम?
Usually NOT preventable! Occurs during fetal development (4-8 weeks)। Unknown cause in most cases। If familial या syndromic: genetic counseling। Prenatal detection: sometimes on ultrasound (but often missed)। Avoid teratogens during pregnancy। Folic acid may help। BUT - most cases sporadic and unavoidable। Focus: early diagnosis and treatment after birth!
Parent की role? / माता-पिता क्या करें?
CRITICAL role! (1) Early intervention - don't delay (2) Splint compliance - MUST wear as directed (3) Therapy consistency - practice exercises (4) Regular follow-ups (5) Emotional support - positive attitude (6) Advocacy - school, activities (7) Education - learn about condition (8) Support groups (9) Adaptation - help child adapt (10) Celebrate milestones! Parental involvement = treatment success। Dr. Gaurav Jain guides families!
📞 Dr. Gaurav Jain से Consult करें - Indore!
📞 Consult Dr. Gaurav Jain - Indore!
Radial Club Hand Expert | Centralization Surgery | Pollicization Specialist Radial Club Hand Expert | Centralization Surgery | Pollicization Specialist
📞 अभी Call करें 📞 Call Now