
Pediatric Fractures – बच्चों में हड्डी टूटना
Pediatric Fractures – Bone Injuries in Children
बच्चे की हड्डियाँ अलग होती हैं – सही तरीके से, सही समय पर इलाज बहुत जरूरी
Children’s bones are different – timely, child-specific fracture care is essential
बच्चों की हड्डी के फ्रैक्चर – वयस्क से कैसे अलग?
How Are Pediatric Fractures Different from Adults?
बच्चे की हड्डी ज़्यादा लचीली, आसपास की झिल्ली (periosteum) मोटी और ग्रोथ प्लेट (growth plate) सक्रिय होती है। इसी वजह से fracture की pattern, treatment और healing, वयस्कों से अलग होती है – इसी के अनुसार योजना बनाना जरूरी है।
मुख्य अंतर
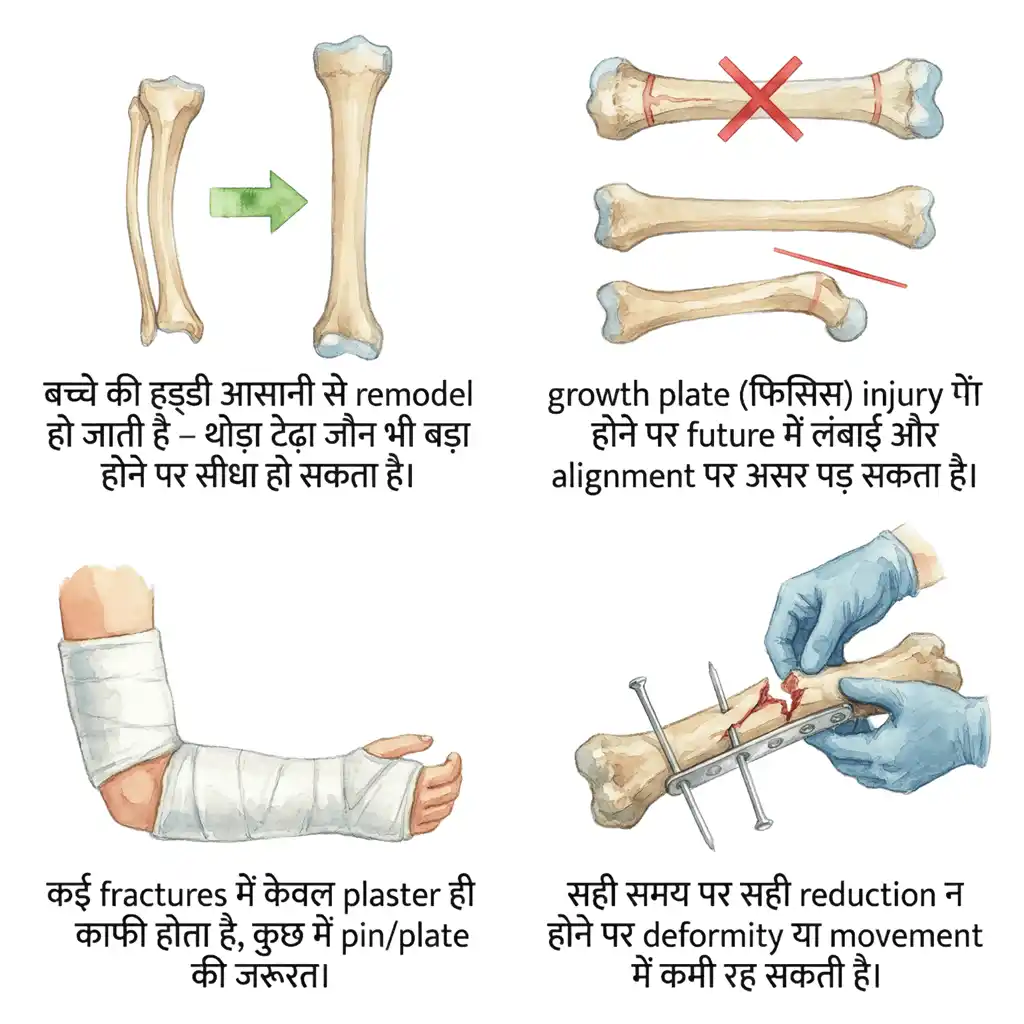
• बच्चे की हड्डी आसानी से remodel हो जाती है – थोड़ा टेढ़ा जौन भी बड़ा होने पर सीधा हो सकता है।
• growth plate (फिसिस) injury होने पर future में लंबाई और alignment पर असर पड़ सकता है।
• कई fractures में केवल plaster ही काफी होता है, कुछ में pin/plate की जरूरत।
• सही समय पर सही reduction न होने पर deformity या movement में कमी रह सकती है।
कब फ्रैक्चर का संदेह करें?
• गिरने / चोट के बाद बच्चा हाथ/पैर चलाने से मना करे।
• सूजन, अचानक deformity या bruise दिखे।
• joint के पास बहुत tenderness, बच्चा उस arm/leg का उपयोग बंद कर दे (toddler fracture आदि)।
• कोई भी doubt हो तो “sprain होगा” मानकर टालने के बजाय X-ray और evaluation ज़रूरी है।
त्वरित तथ्य
Children’s bones are softer, more elastic and surrounded by a thick periosteum, with active growth plates. This makes fracture types, treatment choices and healing patterns quite different from adults.
Key Differences
• Excellent remodelling capacity – some angulation can correct with growth.
• Growth plate injuries can affect future length and alignment.
• Many fractures can be treated safely with plaster alone; some need pins/plates.
• Poorly treated fractures may lead to deformity or restricted movement.
When to suspect a fracture?
• After fall/injury, child refuses to use the limb.
• Visible swelling, deformity or bruising.
• Tenderness near joints; toddler suddenly refuses to walk or limps.
• Do not assume “just a sprain” – timely X-ray and assessment are important.
Quick Facts
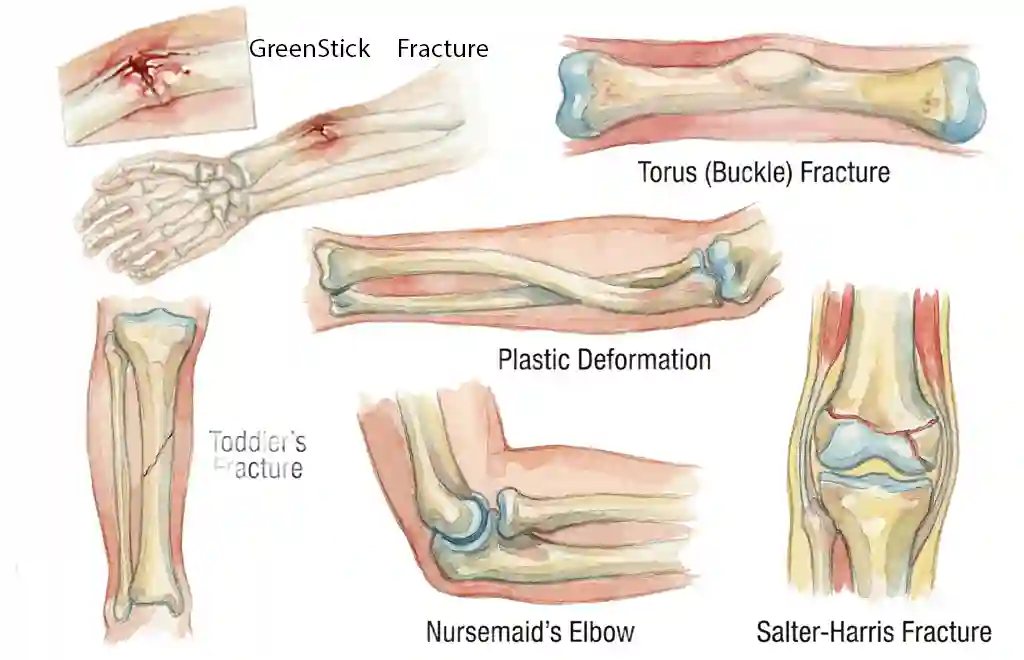
बच्चों में आम प्रकार के फ्रैक्चर
Common Types of Pediatric Fractures
ऊपरी हाथ और कलाई के फ्रैक्चर
1. Distal Radius / दोनों हड्डियों के फ्रैक्चर
• गिरकर हाथ के बल लगने पर सबसे common fracture।
• कई बार सिर्फ greenstick या buckle (torus) fracture होता है – stable pattern।
• plaster से बढ़िया इलाज, severe angulation में manipulation + casting या pinning।
2. Supracondylar Humerus Fracture (कोहनी के ऊपर)
• बच्चों में elbow के पास सबसे महत्वपूर्ण fracture – nerve और vessel injury का risk।
• अक्सर surgery (closed reduction + percutaneous pinning) की जरूरत।
• देरी या गलत treatment से stiffness, deformity या जटिलता हो सकती है।
3. Lateral Condyle / Medial Epicondyle etc.
• elbow के भीतर joint surface से जुड़े fracture – growth plate और cartilage शामिल।
• ऐसे fracture में सटीक alignment बेहद जरूरी – अक्सर surgery से fixation।
नीचे के पैर और अन्य फ्रैक्चर
4. Tibia / Fibula (Leg Bone) Fracture
• road traffic injury, गिरने या sports से।
• छोटे बच्चों में toddler fracture subtle हो सकता है – X-ray initial में normal दिख सकता है, clinical suspicion ज़रूरी।
• plaster, functional brace या intramedullary fixation स्थिति अनुसार।
5. Clavicle, Humerus Shaft, Femur etc.
• clavicle fracture बहुत common और अक्सर sling से heal।
• femur fracture में age के अनुसार traction, spica cast, flexible nails या plating की planning।
• polytrauma या head injury के साथ होने पर ICU level care की जरूरत हो सकती है।
Growth Plate (Physeal) Injuries
• Salter-Harris classification के अनुसार grading।
• गलत treatment या missed injury से future में limb length discrepancy या deformity हो सकती है।
• इसलिए joint के पास fracture को हमेशा special ध्यान से evaluate करना चाहिए।
Upper Limb & Wrist Fractures
1. Distal Radius / Forearm Fractures
• Very common after fall on outstretched hand.
• Buckle/torus and greenstick fractures are typical in children.
• Managed with casting; displaced cases may need manipulation and K-wire fixation.
2. Supracondylar Humerus Fracture
• Most important pediatric elbow fracture; risk of nerve/artery injury.
• Often requires closed reduction and percutaneous pinning.
• Delay or improper treatment can cause deformity or stiffness.
3. Lateral Condyle & Other Elbow Fractures
• Involve joint surface and growth plate.
• Need precise alignment; frequently treated surgically to avoid long-term deformity.
Leg & Other Fractures
4. Tibia / Fibula Fractures
• Seen after falls, sports or road traffic injuries.
• Toddler fractures may be subtle; high clinical suspicion needed.
• Treated with casts, functional bracing or nails depending on age and pattern.
5. Clavicle, Humerus Shaft, Femur
• Clavicle fractures often treated non-operatively with sling.
• Femur fractures: traction, spica cast, flexible nails or plates based on age/weight and pattern.
• Polytrauma cases may need multidisciplinary and ICU care.
Growth Plate (Physeal) Injuries
• Classified using Salter–Harris system.
• Missed/poorly treated injuries may cause growth arrest and deformity.
• Any fracture near joint must be evaluated carefully for physeal involvement.
Pediatric Fractures – इलाज की मुख्य बातें
Management of Pediatric Fractures – Key Principles
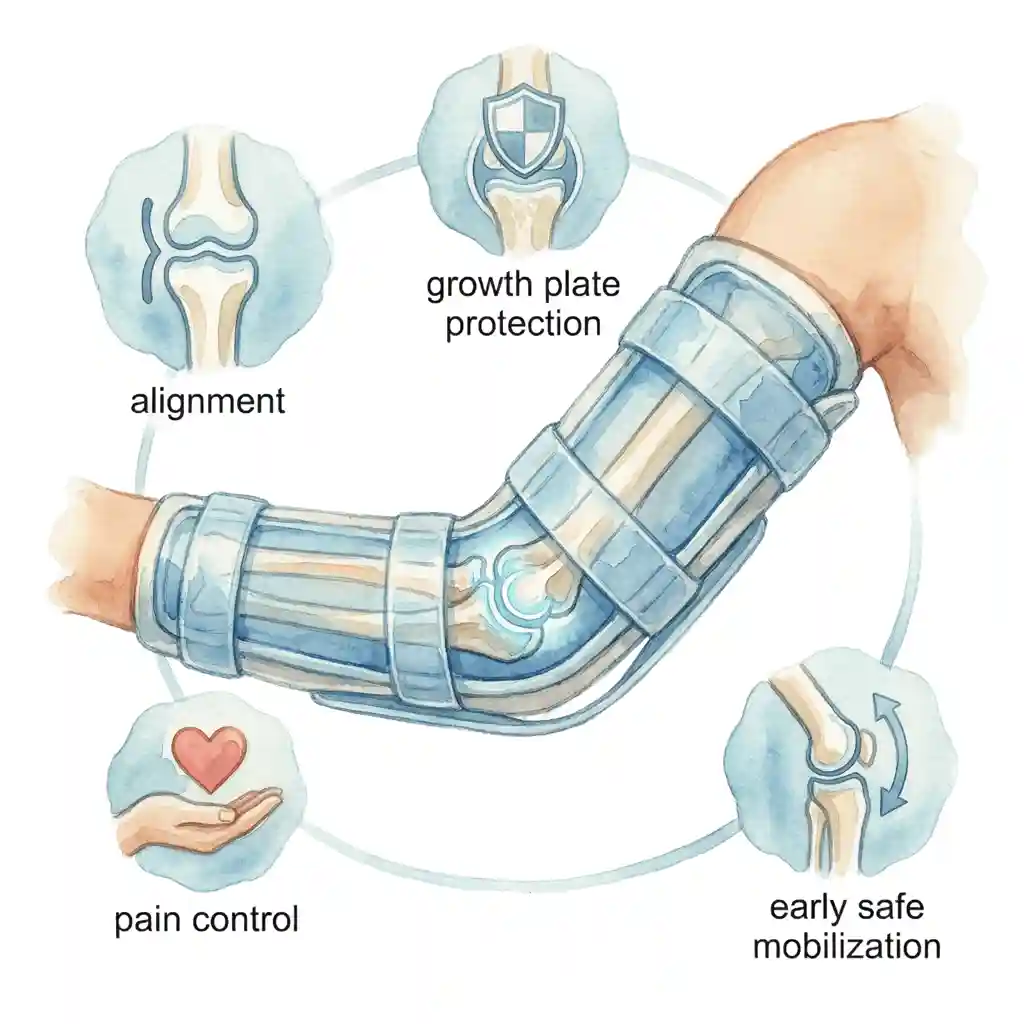
सिर्फ plaster नहीं – alignment, growth plate और function पर ध्यान
बच्चों के फ्रैक्चर में treatment का लक्ष्य है – सही alignment, growth plate की सुरक्षा, दर्द नियंत्रण और जल्दी safe mobilization। हर fracture के लिए अलग योजना बनती है।
प्राथमिक (first aid) क्या करें?
1. Immobilization और दर्द नियंत्रण
• suspected fracture में limb को स्थिर रखें – कपड़ा, cardboard या splint से support दें।
• बहुत ज़्यादा pressure देने या खुद खींचकर सीधा करने की कोशिश न करें।
• simple pain relief (जैसे paracetamol) doctor की सलाह से दे सकते हैं।
2. जल्द से जल्द X-ray और assessment
• nearby center में X-ray, फिर pediatric orthopedic opinion।
• open fracture (घाव के साथ), severe deformity, fingers/ toes नीले/ ठंडे/ senseless हों तो emergency।
मुख्य treatment विकल्प
1. Plaster Cast / Splint
• अधिकांश stable या minimally displaced fractures में plaster काफी।
• careful casting technique – pressure points, circulation और skin care पर ध्यान।
• follow-up X-ray से alignment और healing की निगरानी।
2. Closed Reduction + Percutaneous Fixation
• anesthesia में fracture को सही position में लाकर छोटे pin (K-wire) या elastic nails से stabilize।
• supracondylar humerus, कुछ forearm और physeal fractures में common technique।
• छोटे incisions, कम soft tissue damage, जल्दी recovery।
3. Open Reduction & Internal Fixation
• जब closed तरीकों से सही alignment न बने या open fracture हो।
• plate, screws या special implants से fixation – बच्चे की उम्र और growth को ध्यान में रखकर implant चुना जाता है।
• infection, stiffness आदि से बचने के लिए strict protocol।
4. Rehabilitation & Follow-up
• cast हटने के बाद gentle physiotherapy, stiffness और weakness कम करने के लिए।
• growth plate injury या complex fractures में long-term follow-up – length, alignment और joint function की निगरानी।
डॉ. गौरव जैन की भूमिका
- child-friendly assessment और fracture pattern की सटीक पहचान
- stable cases में plaster, complex cases में minimally invasive surgery की योजना
- growth plate protection और deformity prevention पर विशेष ध्यान
- parents को clear explanation – क्या normal है, क्या risk है, long-term योजना क्या है
More than just a plaster – protect growth and function
Goals in pediatric fracture care are safe alignment, growth plate protection, pain control and early safe mobilization, tailored to each fracture type.
Initial Management
1. Immobilization & Pain Relief
• Keep the injured limb supported and still with a temporary splint.
• Avoid forceful attempts to straighten at home.
• Simple analgesics (like paracetamol) as per medical advice.
2. Early X-ray & Specialist Evaluation
• Obtain X-rays and seek pediatric orthopedic opinion early.
• Open fractures, severe deformity or compromised circulation are emergencies.
Main Treatment Options
1. Plaster Cast / Splint
• Standard care for many stable or minimally displaced fractures.
• Careful cast application to avoid pressure sores and circulation problems.
• Follow-up X-rays monitor position and healing.
2. Closed Reduction & Percutaneous Fixation
• Fracture reduced under anesthesia and fixed with K-wires or flexible nails.
• Common for supracondylar humerus, certain forearm and physeal fractures.
• Minimally invasive, preserves soft tissues and speeds recovery.
3. Open Reduction & Internal Fixation
• Used when closed methods fail or in complex/open injuries.
• Plates, screws or specific pediatric implants chosen considering growth.
• Strict protocols to reduce infection and stiffness.
4. Rehabilitation & Follow-up
• Physiotherapy after cast removal to regain motion and strength.
• Long-term follow-up in growth plate/intra-articular fractures to monitor length and alignment.
Role of Dr. Gaurav Jain
- Child-friendly fracture assessment and pattern-based planning
- Plaster management for stable fractures and minimally invasive fixation for complex ones
- Strong focus on growth plate protection and deformity prevention
- Clear communication with parents about expectations and long-term follow-up
प्लास्टर के दौरान और बाद में – माता-पिता के लिए सुझाव
During & After Cast – Parent Tips and Recovery
Plaster / Cast की देखभाल
1. Cast को सूखा और साफ रखें
• cast के अंदर पानी या तेल न जाने दें – infection और skin maceration का risk बढ़ता है।
• itching हो तो अंदर पेन, scale या stick न डालें – skin injury का खतरा।
2. सूजन और circulation पर नज़र
• fingers/toes बहुत सूजें, नीले या ठंडे हों, child excess pain बताए – तुरंत अस्पताल से संपर्क।
• cast के किनारों पर redness या घाव दिखे तो review करवाएँ।
3. Activity guidance
• doctor की सलाह के अनुसार weight-bearing या sling use करें।
• गिरने/टकराने से बचाएँ, खासकर पहले 1–2 हफ्ते।
Cast हटने के बाद
• stiffness और हल्की कमजोरी normal – 2–4 हफ्तों में अक्सर काफी सुधार।
• simple home exercises या physiotherapy से movement और strength लौटती है।
• कुछ fractures में sports return के लिए stepwise योजना – direct heavy sports में न कूदें।
कब तुरंत emergency में जाएँ?
• accident के बाद deformity, severe pain या child limb use न कर पा रहा हो।
• cast के बाद fingers/toes senseless, very pale/blue या extreme pain हो।
• high fever, foul smell या pus जैसे signs cast से आएँ।
ऐसे सभी मामलों में delay न करें।
Cast Care at Home
1. Keep Cast Dry & Clean
• Avoid water entering the cast; protect during baths.
• Do not insert pens or sticks for itching – risk of skin injury and infection.
2. Watch for Swelling & Colour
• Excessive swelling, bluish or cold fingers/toes with severe pain – urgent review.
• Redness, sores or bad smell from cast need evaluation.
3. Activity and Protection
• Follow weight-bearing and sling instructions strictly.
• Prevent falls and rough play, especially in early healing phase.
After Cast Removal
• Mild stiffness, thinner limb and dry skin are common and usually temporary.
• Gentle exercises and physiotherapy help restore function.
• Sports return should be gradual, following your surgeon’s timeline.
When to Seek Emergency Care?
• Post-injury visible deformity or inability to move limb.
• After casting: severe pain, pale/blue or numb fingers/toes.
• High fever, foul odour or discharge from cast.
Do not delay in such situations.
वीडियो – फ़्रैक्चर्स की जानकारी
Fractures – Complete Explanation
बच्चों में फ्रैक्चर के कारण, जांच और इलाज की पूरी जानकारी – डॉ. गौरव जैन द्वारा।
Causes, diagnosis and treatment of Fractures in children — explained by Dr. Gaurav Jain.

Pediatric Fractures – अक्सर पूछे जाने वाले प्रश्न
Pediatric Fractures – Frequently Asked Questions
क्या बच्चों में fracture ज्यादा खतरनाक होता है? / Are fractures more dangerous in children?
हर fracture dangerous नहीं होता, बल्कि बच्चों में healing और remodelling अच्छी होती है। लेकिन growth plate के पास और joint के अंदर वाले fractures में सही समय पर सही treatment न मिलने पर future deformity या function पर असर पड़ सकता है, इसलिए इन्हें lightly नहीं लेना चाहिए।
Sprain और fracture में कैसे फर्क समझें? / How to differentiate sprain from fracture?
कभी-कभी केवल clinical exam से clear नहीं होता। यदि बच्चा limb चलाने से पूरी तरह मना करे, localized bone tenderness हो, deformity दिखे या weight-bearing न कर पा रहा हो, fracture का doubt अधिक होता है। doubt होने पर X-ray आवश्यक है – बिना X-ray देखे final निर्णय नहीं करना चाहिए।
क्या हर fracture में plaster जरूरी है? / Is plaster required for every fracture?
कई fractures में हाँ, plaster या splint जरूरी होता है, लेकिन कुछ non-displaced या stable fractures में removable splint या functional brace भी options हैं। वहीं कुछ गंभीर fractures में plaster के साथ-साथ internal fixation (pins/plates) की भी जरूरत पड़ती है – यह fracture की type और stability पर निर्भर करता है।
बच्चों में fracture कितनी जल्दी जुड़ता है? / How fast do children’s fractures heal?
यह उम्र, fracture site और pattern पर depend करता है। अक्सर upper limb fractures 3–4 weeks में और कुछ lower limb fractures 4–6 weeks या थोड़ा अधिक समय में clinically heal हो जाते हैं। लेकिन radiological healing और full strength आने में इससे ज्यादा समय लग सकता है, इसलिए activity timing डॉक्टर तय करते हैं।
क्या बच्चों में surgery avoid कर सकते हैं? / Can surgery usually be avoided in children?
कई pediatric fractures सिर्फ plaster से ही ठीक हो जाते हैं, लेकिन कुछ specific fractures – जैसे displaced supracondylar humerus, unstable forearm fractures, certain femur fractures – में surgery safer और बेहतर alignment देती है। लक्ष्य surgery से बचना नहीं, बल्कि best functional result पाना होता है।
क्या pins/plates बच्चा बड़ा होने तक शरीर में रह सकते हैं? / Do pins and plates need removal?
K-wires आमतौर पर कुछ हफ्तों/ महीनों में हड्डी जुड़ने के बाद निकाल दिए जाते हैं। plates/screws को removal की आवश्यकता fracture type, location, symptoms और growth पर depend करती है। कुछ implants लम्बे समय तक सुरक्षित रह सकते हैं, कुछ में later removal plan किया जाता है – यह individualized निर्णय है।
क्या fracture के बाद physiotherapy जरूरी है? / Is physiotherapy necessary after fracture?
कई छोटे बच्चों में केवल normal daily use से ही movement धीरे-धीरे वापस आ जाती है। लेकिन joint के पास के fractures, लंबे time immobilization या surgery के बाद stiffness और weakness ज्यादा हो सकती है – ऐसे में structured physiotherapy और home exercises से recovery तेज और सुरक्षित होती है।
क्या हर fracture में general anesthesia देना पड़ता है? / Is general anesthesia always required?
छोटे manipulations, splinting या simple casting अक्सर sedation या local measures से हो सकते हैं। लेकिन major closed reduction, pinning या surgery के लिए बच्चों में general anesthesia अक्सर safest और comfortable विकल्प होता है। Anesthesia team child-specific risk assessment करती है।
क्या fracture के बाद हाथ/पैर छोटा या टेढ़ा रह सकता है? / Can the limb become short or crooked later?
अधिकांश सही तरीके से treated fractures में long-term length और alignment normal रहता है। लेकिन growth plate injury, severe angulation या malunion होने पर limb length discrepancy या deformity हो सकती है। इसी वजह से joint के पास वाले fractures में long-term follow-up और time-to-time X-ray important हैं।
क्या बच्चा future में sports कर पाएगा? / Will my child be able to play sports in future?
ज्यादातर बच्चों में fracture ठीक होने के बाद और proper rehab के साथ normal sports participation possible होता है। high-impact या competitive sports में return से पहले surgeon clearance और stepwise progression ज़रूरी है, खासकर joint या growth plate fractures के बाद।
Fracture के बाद permanent pain का risk है? / Is there risk of permanent pain?
सही alignment, अच्छी healing और proper rehab होने पर permanent pain uncommon है। chronic pain अक्सर malunion, joint incongruity, infection या untreated soft tissue injury से जुड़ा होता है – इसलिए प्रारंभिक treatment और follow-up quality पर बहुत निर्भर करता है।
Fracture के बाद दुबारा टूटने का खतरा बढ़ जाता है? / Does a bone break more easily again?
Initial healing के बाद कुछ समय तक fracture site थोड़ा sensitive रह सकता है, पर fully healed होने के बाद bone strength सामान्य या कभी-कभी आसपास की bone से भी अधिक हो सकती है। बार-बार fractures हों तो vitamin D deficiency या अन्य bone problems evaluate करनी चाहिए।
Cast हटने के बाद बच्चा डर-डर कर limb उपयोग करता है – क्या करें? / Child is afraid to use limb after cast removal – what to do?
यह बहुत common है – stiffness, weakness और डर के कारण। gentle reassurance, खेल-खेल में exercises और धीरे-धीरे weight-bearing से confidence वापस आता है। यदि limp, significant pain या movement में कमी बनी रहे तो पुनः evaluation और physiotherapy useful है।
क्या fracture के बाद diet में कुछ खास देना चाहिए? / Any special diet after fracture?
संतुलित diet – पर्याप्त protein, calcium, vitamin D और hydration – healing में मदद करती है। अत्यधिक sugary drinks या junk food से बचें। यदि child underweight हो या vitamin D deficiency हो, तो doctor supplements सलाह दे सकते हैं।
क्या घर पर पुराने orthopaedic बेल्ट/ splint उपयोग कर सकते हैं? / Can we use old splints at home without prescription?
Self-application of splints या braces without proper assessment से fracture का pattern worsen हो सकता है या joint stiff हो सकते हैं। इसलिए design, size और duration हमेशा pediatric orthopaedic advice से तय करना चाहिए, पुराने devices blindly reuse नहीं करने चाहिए।
क्या बार-बार fracture होना normal है? / Is repeated fracture normal in a child?
बहुत active बच्चे में 1–2 चोटें जीवन में होना uncommon नहीं, पर बार-बार कई fractures होना normal नहीं माना जाता। ऐसे में vitamin D deficiency, nutritional issues, bone disease या repeated trauma (non-accidental injury) का evaluation करना आवश्यक हो सकता है।
Fracture के कितने समय बाद X-ray repeat करना चाहिए? / How often are repeat X-rays needed?
यह fracture type पर depend करता है। कई stable fractures में 1–2 follow-up X-rays पर्याप्त हैं, जबकि unstable, reduced या physeal fractures में alignment और growth का आकलन करने के लिए अधिक frequent X-rays की आवश्यकता हो सकती है। Doctor radiation benefit–risk balance को ध्यान में रखकर schedule तय करते हैं।
किस specialist को दिखाएँ? / Which specialist should we consult for pediatric fractures?
बच्चों के fractures के लिए Pediatric Orthopedic Surgeon सबसे उपयुक्त specialist हैं, क्योंकि उन्हें growth plate, remodelling और child-specific implants का विशेष अनुभव होता है। इंदौर में डॉ. गौरव जैन ऐसे fractures का comprehensive, evidence-based उपचार प्रदान करते हैं।
Parents की सबसे महत्वपूर्ण भूमिका क्या है? / What is the most important role of parents?
Timely hospital पहुँचाना, instructions को ध्यान से समझना, cast/brace care सही तरह करना, follow-up miss न करना और बच्चे को emotional support देना – यही सबसे महत्वपूर्ण भूमिका है। unnecessary fear से बचते हुए scientific जानकारी पर भरोसा करना child के लिए best है।
क्या दूसरी राय (second opinion) लेना ठीक है? / Is it okay to take a second opinion?
हाँ, विशेषकर जब major surgery, growth plate injury या long-term effect वाले fracture की बात हो। second opinion से parents को decision के प्रति अधिक विश्वास मिलता है। बस यह ध्यान रहे कि opinions pediatric ortho specialists और evidence-based guidelines पर आधारित हों।
Pediatric Fractures के लिए डॉ. गौरव जैन – इंदौर में विशेषज्ञ इलाज
Specialist Care for Pediatric Fractures in Indore – Dr. Gaurav Jain
बच्चों के fractures के लिए child-friendly वातावरण, accurate X-ray planning, plaster से लेकर minimally invasive surgery तक – एक ही जगह पर comprehensive pediatric orthopedic सेवा। Child-friendly environment, accurate X-ray based planning, from plaster casts to minimally invasive surgery – complete pediatric fracture care under one roof.
कॉल करें Call Now