
टेढ़े पैर – Bow Legs / Knock Knees
Bow Legs & Knock Knees in Children
कब नॉर्मल है, कब बीमारी – आसान भाषा में समझें, सही समय पर इलाज पाएं
Understand what is normal vs abnormal and when treatment is needed for your child’s leg shape
Bow Legs / Knock Knees – क्या नॉर्मल, क्या नहीं?
Bow Legs / Knock Knees – Normal vs Problem
छोटे बच्चों में पैरों का थोड़ा टेढ़ापन अक्सर नॉर्मल ग्रोथ का हिस्सा होता है। लेकिन कभी-कभी यही टेढ़ापन ज़्यादा, असमान या बढ़ता हुआ हो तो वह बीमारी या deformity हो सकती है जिसे जांच और इलाज की जरूरत होती है।
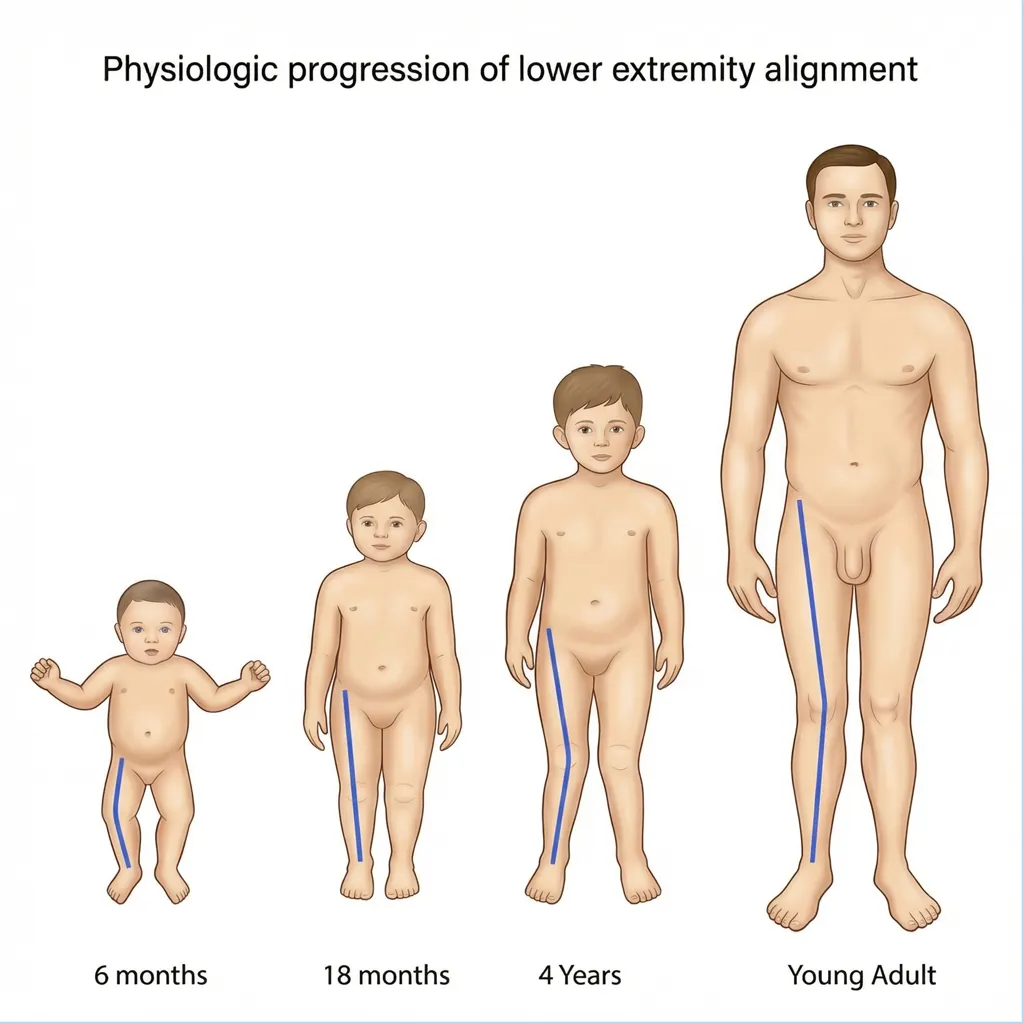
आम पैटर्न (Normal Growth Pattern)
• जन्म के बाद – हल्का bow legs (O-शेप) नॉर्मल।
• लगभग 18–24 महीने – सीधा लगने लगता है।
• 3–4 साल – हल्का knock knees (X-शेप) नॉर्मल।
• 7–8 साल तक – अधिकांश बच्चे के पैर लगभग सीधे हो जाते हैं।
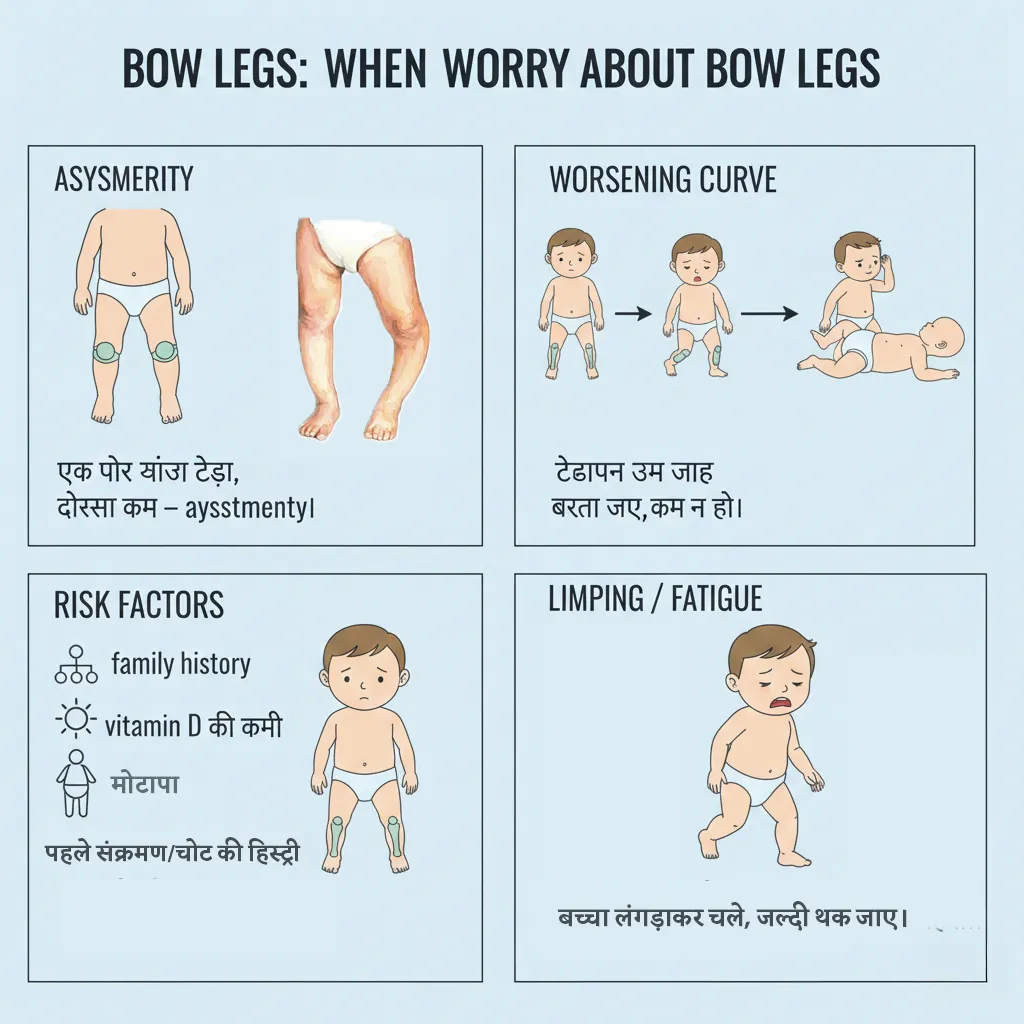
कब चिंता करनी चाहिए?
• एक पैर ज़्यादा टेढ़ा, दूसरा कम – asymmetry।
• टेढ़ापन उम्र के साथ बढ़ता जाए, कम न हो।
• बच्चा लंगड़ाकर चले, जल्दी थक जाए।
• family history, vitamin D की कमी, मोटापा, पहले संक्रमण/चोट की हिस्ट्री।
ऐसे में pediatric orthopedic specialist को अवश्य दिखाएँ।
स्टैट्स (संक्षिप्त)
Some bowing or knock-knee appearance in young children is a normal part of growth. However, if the deformity is severe, one-sided, worsening or persisting, it may be a pathological deformity needing evaluation and treatment.
Typical Physiological Pattern
• Newborn – mild bow legs (O-shape) is normal.
• Around 18–24 months – legs become straighter.
• 3–4 years – mild knock knees (X-shape) is common.
• By 7–8 years – most children have near straight alignment.
When to be concerned?
• Deformity is more on one side (asymmetrical).
• Bowing/knock knees increase with age instead of improving.
• Child limps, trips often or tires easily.
• History of rickets, infection, trauma or strong family history.
In such situations, consult a pediatric orthopedic specialist.
Quick Facts
Bow Legs / Knock Knees – प्रकार और कारण
Types & Causes of Bow Legs / Knock Knees
मुख्य प्रकार
1. Bow Legs (Genu Varum)
पैरों के बीच गैप, घुटने दूर–दूर, टखने पास–पास। छोटे बच्चों में हल्का bow legs सामान्य, लेकिन बड़ा बच्चे में ज़्यादा bow legs – खासकर एक तरफ – बीमारी (rickets, Blount disease, post-trauma) का संकेत हो सकता है।
2. Knock Knees (Genu Valgum)
घुटने आपस में टकराते, टखनों में गैप रहता है। 3–7 साल के बच्चों में हल्का X-shape नॉर्मल है, लेकिन बहुत ज़्यादा, असमान या 8–10 साल के बाद भी रहे तो इलाज की जरूरत हो सकती है।
3. Pathological Deformity
Rickets (विटामिन D की कमी), Blount disease (growth plate की बीमारी), infection या fracture के बाद हड्डी टेढ़ी जमी हो – ये सब pathological deformity हैं, जिन्हें केवल “इंतज़ार” से ठीक नहीं माना जाता।
4. Secondary Changes
लंबे समय तक untreated deformity से joint पर असमान भार पड़ता है – आगे चलकर घुटने में दर्द, चाल बिगड़ना, जल्दी arthritis का जोखिम बढ़ता है – इसलिए समय पर correction महत्वपूर्ण है।
आम कारण
• Physiological – प्राकृतिक ग्रोथ पैटर्न, खुद ठीक हो जाता।
• Rickets – विटामिन D / कैल्शियम की कमी से मुलायम हड्डियाँ।
• Blount disease – टिबिया के growth plate की बीमारी, खासकर मोटे बच्चों में।
• Post-traumatic – fracture गलत एंगल पर भरना।
• Genetic / metabolic – कम पाए जाने वाले कारण।
Main Types
1. Bow Legs (Genu Varum)
Legs curved outward, knees far apart, ankles close. Mild bowing in toddlers is normal, but marked bowing in older child, especially one-sided, suggests pathology like rickets or Blount disease.
2. Knock Knees (Genu Valgum)
Knees touch or come close while ankles stay apart. Mild knock knees at 3–7 years are physiological, but severe or persistent deformity beyond 8–10 years may need treatment.
3. Pathological Deformity
Due to rickets, Blount disease, previous infection or malunited fracture; these do not usually correct on their own and need proper evaluation and planning.
4. Secondary Joint Problems
Long-standing deformity overloads one side of the knee, leading to pain, abnormal gait and early osteoarthritis in adult life if not corrected in time.
Common Causes
• Physiological – normal age-related variation.
• Rickets – vitamin D / calcium deficiency causing soft bones.
• Blount disease – growth plate disorder of proximal tibia.
• Post-traumatic – malunited fractures affecting alignment.
• Genetic / metabolic bone disorders – less common but important.
जांच और इलाज – Bow Legs / Knock Knees
Evaluation & Treatment – Bow Legs / Knock Knees
हर टेढ़ा पैर सर्जरी से नहीं – सही उम्र में सही योजना!
कई बच्चों में केवल निगरानी, पोषण और फिजियो से सुधार हो जाता है। जबकि pathological deformity में guided growth या deformity correction की जरूरत हो सकती है।
जांच कैसे होती है?
1. क्लिनिकल Assessment
• चलने और खड़े होने की जांच।
• घुटनों के बीच/टखनों के बीच की दूरी मापना।
• जांघ और टांग की alignment देखना, लंबाई का अंतर चेक करना।
2. X-ray + Long Film
• दोनों पैरों का weight-bearing X-ray।
• mechanical axis और deformity कहाँ से आ रही है (femur vs tibia) पता चलता है।
• रिकेट्स, growth plate की समस्या के संकेत भी दिखते हैं।
3. Blood Tests (जब ज़रूरी)
• Vitamin D, calcium, phosphate, alkaline phosphatase – rickets का संदेह हो तो।
• अन्य metabolic tests ज़रूरत अनुसार।
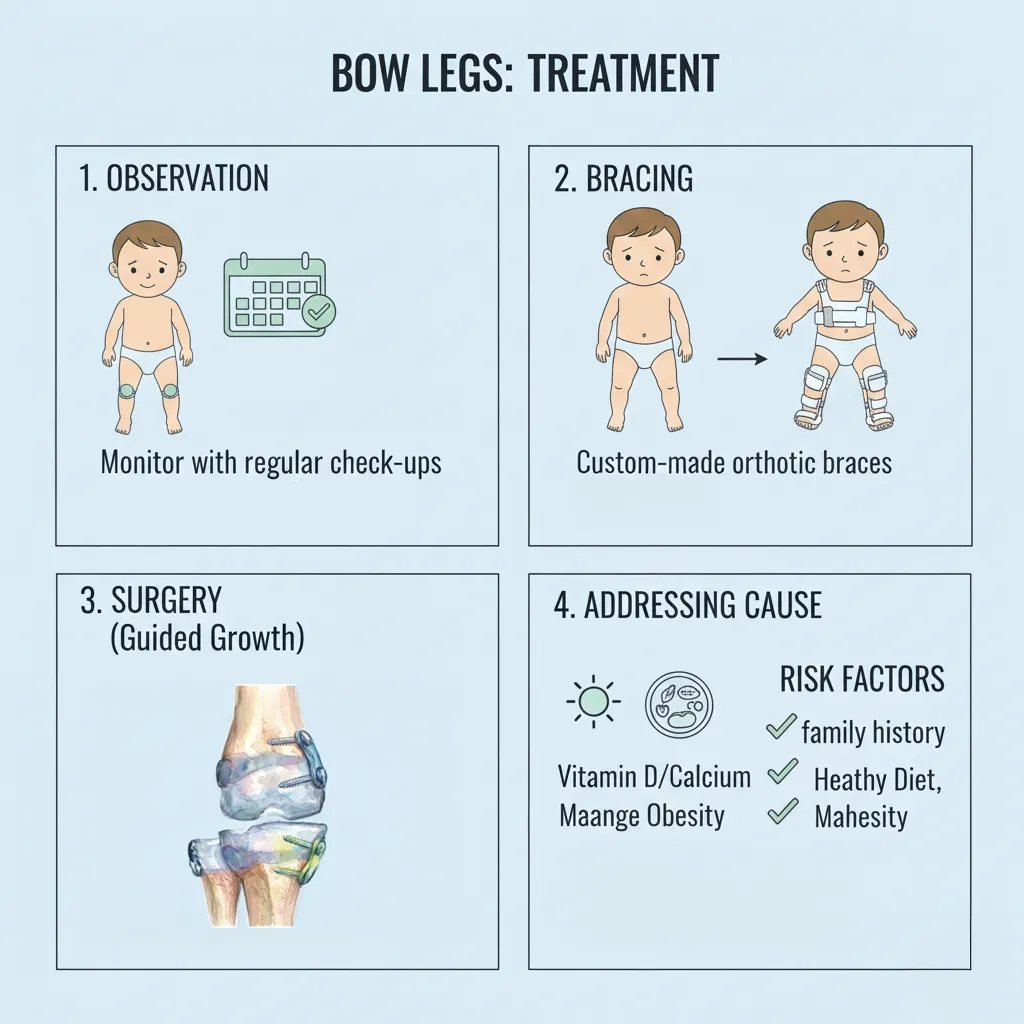
मुख्य उपचार विकल्प
1. Observation & Nutritional Treatment
• physiological bow legs / knock knees में सिर्फ निगरानी और follow-up।
• rickets में vitamin D + calcium सही डोज में, diet counseling।
• lifestyle बदलाव – सूरज की रोशनी, मोटापे को कंट्रोल करना।
2. Guided Growth Surgery
• growing age (आमतौर पर 8–14 साल) में growth plate पर छोटी प्लेट/स्क्रू लगाकर धीरे-धीरे deformity को सीधा करना।
• छोटी चीरे वाली, कम दर्द वाली प्रक्रिया, अक्सर early चलना संभव।
3. Corrective Osteotomy
• बहुत ज्यादा deformity, बहुत late age या growth plate बंद हो चुकी हो।
• हड्डी को सही एंगल पर काटकर प्लेट/स्क्रू से फिक्स किया जाता है।
• deformity तुरन्त सीधी हो जाती है, फिर फिजियो की जरूरत।
4. फिजियोथेरेपी एवं रिहैब
• मसल स्ट्रेंथ बढ़ाने, चाल सुधारने, balance और endurance के लिए।
• surgery के बाद recovery का महत्वपूर्ण हिस्सा।
डॉ. गौरव जैन की भूमिका
- physiological vs pathological deformity की सही पहचान
- उम्र और ग्रोथ के अनुसार guided growth planning
- deformity correction osteotomy और fixation
- लंबी अवधि तक alignment और joint health की निगरानी
Not every crooked leg needs major surgery!
Many children require only observation, nutrition and follow-up, while pathological deformities may need guided growth or corrective osteotomy.
How is assessment done?
1. Clinical Examination
• Gait and standing posture.
• Measuring distance between knees/ankles.
• Checking limb length and alignment of femur and tibia.
2. X-ray & Long Leg Films
• Weight-bearing X-rays of both legs.
• Helps locate site of deformity and measure mechanical axis.
• Shows features of rickets or growth plate disorders.
3. Blood Tests (when needed)
• Vitamin D, calcium, phosphate, ALP for suspected rickets.
• Additional metabolic workup when indicated.
Main Treatment Options
1. Observation & Nutritional Therapy
• For physiological deformities – watchful waiting with periodic review.
• Treat rickets with correct vitamin D and calcium doses.
• Encourage outdoor play and weight control.
2. Guided Growth (Hemiepiphysiodesis)
• In growing children, small plate/screws placed at growth plate to gradually correct deformity.
• Minimally invasive, shorter hospital stay, child walks early with care.
3. Corrective Osteotomy
• For severe deformity or after growth plate closure.
• Bone cut and realigned to correct axis, fixed with plate/screws.
• Deformity corrected immediately, followed by physiotherapy.
4. Physiotherapy & Rehabilitation
• Strengthening muscles, improving gait and balance.
• Essential after surgery to regain confidence and function.
Role of Dr. Gaurav Jain
- Accurate differentiation between physiological and pathological deformities
- Age-appropriate guided growth planning and execution
- Corrective osteotomy and deformity correction surgeries
- Long-term monitoring of alignment and joint health
वीडियो – Bow Legs / Knock Knees की जानकारी
Watch: Bow Legs & Knock Knees – Patient Education Video
बच्चों के टेढ़े पैरों के बारे में सब कुछ समझें – कारण, जांच और इलाज – डॉ. गौरव जैन द्वारा।
Everything you need to know about bow legs & knock knees in children — causes, evaluation and treatment options — explained by Dr. Gaurav Jain.

माता-पिता के लिए टिप्स और भविष्य
Parent Tips & Long-term Outcome
घर पर क्या ध्यान रखें?

1. जूते / स्पेशल जूते
आमतौर पर केवल जूते बदलने से deformity नहीं ठीक होती। कुछ मामलों में orthotic insoles या विशेष जूते सहायक हो सकते हैं, पर यह decision विशेषज्ञ की सलाह से होना चाहिए।
2. पोषण और धूप
संतुलित diet, पर्याप्त vitamin D और calcium, रोज़ कुछ समय धूप में खेलना – हड्डियों के लिए बहुत महत्वपूर्ण है, खासकर अगर पहले rickets रहा हो।
3. वज़न कंट्रोल
मोटापा deformity पर अतिरिक्त भार डालता है, खासकर knock knees में। age-appropriate exercise और diet से healthy weight maintain करना उपयोगी है।
भविष्य और prognosis
• physiological cases में, सही monitoring के साथ आमतौर पर कोई long-term समस्या नहीं होती।
• सही समय पर guided growth / correction से बच्चा सामान्य या लगभग सामान्य सीधी टांगों और अच्छी चाल के साथ बड़ा हो सकता है।
• बहुत देर से इलाज या untreated deformity में future में घुटने का दर्द और arthritis का खतरा बढ़ सकता है।
कब तुरंत डॉक्टर से मिलें?
• बच्चा अचानक ज़्यादा टेढ़ा चलने लगे या दर्द की शिकायत करे।
• एक पैर में ही deformity ज़्यादा हो।
• surgery/plate लगने के बाद अचानक दर्द, सूजन, बुखार या चोट लगे।
ऐसे सभी मामलों में तुरंत संपर्क करना उचित है।
What can parents do at home?
1. Footwear & Braces
Simply changing shoes usually does not correct true deformity. In selected cases, orthotics/braces may support alignment, but this should be guided by your specialist.
2. Nutrition & Sunlight
Balanced diet with adequate vitamin D and calcium and regular sunlight exposure helps maintain healthy bones, especially after rickets treatment.
3. Weight Management
Excess weight strains the knees and can worsen knock knees. Age-appropriate activity and diet help in maintaining healthy weight and joint protection.
Long-term Outcome
• Physiological deformities usually have excellent long-term outcome with simple observation.
• Timely guided growth or corrective surgery allows a child to grow up with near-normal alignment and gait.
• Untreated severe deformities can lead to knee pain and early osteoarthritis in adult life.
When to seek urgent review?
• Sudden worsening of deformity or new-onset pain.
• Marked difference between the two legs.
• After surgery, if there is severe pain, swelling, fever or trauma over the operated limb.
In such situations, contact your doctor immediately.
Bow Legs / Knock Knees – अक्सर पूछे जाने वाले प्रश्न
Bow Legs / Knock Knees – Frequently Asked Questions
क्या छोटे बच्चों में bow legs नॉर्मल है? / Are bow legs normal in infants?
ज्यादातर बच्चे जन्म के समय और पहले 1–2 साल तक हल्के bow legs के साथ होते हैं, जो प्राकृतिक ग्रोथ पैटर्न का हिस्सा है और समय के साथ खुद सुधर जाता है, यदि deformity बहुत ज़्यादा न हो और दोनों पैरों में समान हो।
Knock knees किस उम्र में नॉर्मल माने जाते हैं? / When are knock knees considered normal?
3–4 साल की उम्र के आसपास हल्के knock knees (X-शेप) अक्सर नॉर्मल होते हैं और 7–8 साल तक धीरे-धीरे सीधे हो जाते हैं। अगर deformity बहुत ज़्यादा हो या 8–10 साल के बाद भी बनी रहे तो जांच ज़रूरी है।
मैं कैसे जानूं कि ये नॉर्मल है या बीमारी? / How do I know if it is normal or pathological?
कुछ चेतावनी संकेत हैं – एक पैर ज़्यादा टेढ़ा हो, deformity उम्र के साथ बढ़ती जाए, बच्चा लंगड़ाए या दर्द बताए, family में गंभीर deformity हो, या X-ray पर abnormal findings दिखें। ऐसे में pediatric orthopedic evaluation ज़रूरी है।
क्या रिकेट्स से हमेशा टेढ़े पैर बनते हैं? / Does rickets always cause deformity?
हर rickets का केस deformity तक नहीं पहुंचता, लेकिन untreated या severe rickets में हड्डियाँ मुलायम होने के कारण bow legs या knock knees विकसित हो सकते हैं। इसलिए vitamin D की कमी का सही समय पर इलाज बहुत महत्वपूर्ण है।
क्या सिर्फ calcium और vitamin D से पैर सीधे हो जाएंगे? / Will vitamin D & calcium alone straighten the legs?
यदि deformity का मुख्य कारण rickets हो और ग्रोथ अभी पर्याप्त हो, तो सही dose में vitamin D और calcium देने पर deformity कुछ हद तक सुधर सकती है। लेकिन advanced या पुरानी deformity में केवल दवाओं से पूरा correction संभव नहीं होता, सर्जिकल planning की जरूरत पड़ सकती है।
Guided growth surgery क्या है? / What is guided growth surgery?
Guided growth में बच्चे की growing हड्डी के एक तरफ growth plate पर छोटी प्लेट/स्क्रू लगाकर growth को नियंत्रित किया जाता है, जिससे समय के साथ पैर खुद सीधा हो जाता है। यह कम कट वाली, कम दर्द वाली प्रक्रिया है और अक्सर day-care या छोटा admission होता है।
Guided growth के लिए आदर्श उम्र क्या है? / Ideal age for guided growth?
आमतौर पर guided growth तब सबसे उपयोगी होता है जब growth plate अभी खुली हो – यानी लगभग 8–14 साल (लड़कियों में थोड़ी कम, लड़कों में थोड़ी देर तक)। बहुत छोटे बच्चे या जिनकी ग्रोथ लगभग खत्म हो चुकी हो, उनमें यह विकल्प सीमित हो सकता है।
Corrective osteotomy कब ज़रूरी होती है? / When is corrective osteotomy needed?
बहुत severe deformity, बहुत late age (growth plate बंद), या ऐसी स्थिति जहाँ guided growth से पर्याप्त correction न हो सके – तब corrective osteotomy की आवश्यकता पड़ती है। इसमें हड्डी को सही कोण पर काटकर प्लेट/स्क्रू से फिक्स किया जाता है।
क्या प्लास्टर या ब्रेस से टेढ़े पैर ठीक हो सकते हैं? / Can braces or plaster cure bow legs/knock knees?
पुरानी धारणा के विपरीत, केवल braces या प्लास्टर से सभी deformities ठीक नहीं होतीं। कुछ selected cases में orthosis support दे सकता है, लेकिन pathological deformity में अक्सर guided growth या osteotomy बेहतर और वैज्ञानिक विकल्प होते हैं।
क्या बच्चा नॉर्मल चल और दौड़ पाएगा? / Will my child walk and run normally after treatment?
अधिकांश बच्चों में, यदि deformity सही समय पर और सही तरीके से ठीक की जाए तो वे आगे चलकर नॉर्मल चल, दौड़ और खेलकूद कर सकते हैं। बहुत देर से इलाज या अत्यधिक deformity में कुछ सीमाएँ रह सकती हैं, पर फिर भी deformity कम करके जीवन की गुणवत्ता में बड़ा सुधार संभव होता है।
इलाज के बाद कितना समय फॉलो-अप करना पड़ता है? / How long follow-up is needed?
Guided growth में प्लेट हटने तक और growth खत्म होने तक नियमित X-ray और OPD विज़िट जरूरी हैं। osteotomy के बाद भी alignment और joint health देखने के लिए कुछ वर्षों तक follow-up रखना फायदेमंद है।
अगर इलाज न कराएँ तो आगे क्या दिक्कत हो सकती है? / What happens if we don’t treat severe deformity?
यदि deformity बहुत ज़्यादा हो और untreated रही तो बड़े होने पर joint पर असमान भार से घुटने में दर्द, चाल बिगड़ना, जल्दी arthritis और cosmetic चिंता हो सकती है। इसलिए केवल cosmetic नहीं, functional कारणों से भी correction की सलाह दी जाती है।
सर्जरी के बाद बच्चा स्कूल कब जा सकता है? / When can my child return to school after surgery?
Guided growth जैसी छोटी प्रक्रिया के बाद अक्सर कुछ दिनों में सामान्य गतिविधियाँ और 1–2 हफ्तों में स्कूल संभव होता है। osteotomy जैसी बड़ी सर्जरी में यह समय अधिक हो सकता है, जो individual case और डॉक्टर की सलाह पर निर्भर करता है।
क्या फिजियोथेरेपी ज़रूरी है? / Is physiotherapy necessary?
हाँ, विशेषकर osteotomy या बड़ी correction के बाद। फिजियो से मसल स्ट्रेंथ, joint की मूवमेंट, चाल और confidence वापस आने में मदद मिलती है। guided growth में भी activity guidance और exercises फायदेमंद रहती हैं।
क्या बच्चा future में खेल-कूद और sports कर पाएगा? / Can my child play sports in future?
अधिकांश corrected deformities में, healing हो जाने और डॉक्टर से clearance मिलने के बाद बच्चा regular games और sports में भाग ले सकता है। high-impact या competitive sports के लिए specialist से individualized सलाह लेना बेहतर है।
क्या यह समस्या hereditary हो सकती है? / Is it hereditary?
कुछ मामलों में family में टेढ़े पैरों का pattern दिख सकता है, खासकर metabolic या genetic bone diseases में। लेकिन अधिकांश physiological bow legs/knock knees में कोई स्पष्ट hereditary बीमारी नहीं पाई जाती, फिर भी family history evaluation महत्त्वपूर्ण है।
क्या हमें second opinion लेना चाहिए? / Should we take a second opinion?
कभी भी कोई major surgery plan हो, parents के लिए second opinion लेना बिल्कुल स्वीकार्य है। यह आपको निर्णय के प्रति अधिक आश्वस्त और comfortable महसूस कराता है, बशर्ते दोनों opinions evidence-based और pediatric orthopedics स्पेशलिस्ट से हों।
किस specialist को दिखाएँ? / Which specialist should we consult?
टेढ़े पैर, bow legs या knock knees के लिए Pediatric Orthopedic Surgeon सबसे उपयुक्त विशेषज्ञ हैं। इंदौर में डॉ. गौरव जैन बच्चों की deformity correction, guided growth और osteotomy में विशेष अनुभव रखते हैं।
क्या deformity दोबारा वापस आ सकती है? / Can deformity recur after correction?
कुछ बच्चों में, खासकर अगर growth बाकी हो या underlying disease active हो (जैसे rickets, Blount), तो कुछ हद तक deformity दोबारा बढ़ सकती है। इसी कारण नियमित follow-up और X-ray monitoring बहुत जरूरी है ताकि समय पर दुबारा हस्तक्षेप किया जा सके।
माता-पिता की सबसे महत्वपूर्ण भूमिका क्या है? / What is the most important role of parents?
समय पर दिखाना, सलाह समझना, follow-up मिस न करना, दवाइयाँ और exercises regular करवाना – यही सबसे महत्वपूर्ण योगदान है। चिंता छुपाने के बजाय खुलकर पूछना और वैज्ञानिक जानकारी पर भरोसा रखना बच्चे के लिए सबसे सुरक्षित है।
Bow Legs / Knock Knees के लिए डॉ. गौरव जैन से परामर्श – इंदौर
Consult Dr. Gaurav Jain in Indore for Bow Legs / Knock Knees
बच्चों के टेढ़े पैरों की सटीक जांच, X-ray planning, guided growth और deformity correction सर्जरी – विशेषज्ञ बाल हड्डी रोग उपचार। Comprehensive evaluation, X-ray based planning, guided growth and deformity correction surgery for children with bow legs / knock knees.
कॉल करें Call Now